


In Spain, around one million people have glaucoma. More than half of them are unaware of it. By the time the damage becomes noticeable in everyday life, part of the optic nerve has already been irreversibly damaged. That is why glaucoma is not managed by waiting for symptoms to appear: it is managed through early diagnosis, active monitoring and treatment tailored to each individual case.
At Dr Ali Nowrouzi’s practice in Marbella, the treatment of glaucoma combines high-precision diagnostic technology with a range of treatment options: ranging from SLT laser treatment and MIGS (Micro-Invasive Glaucoma Surgery) techniques to surgery combined with premium intraocular lenses. Dr Nowrouzi, who is FEBOS-CR certified and recognised as a Top Doctor for 2024, 2025 and 2026, sees patients at Clínica Premium Marbella, Quirónsalud, Hospital Ochoa and Hospiten Estepona.

What is glaucoma and why do half of all cases remain undiagnosed?
Glaucoma is not a single disease but a group of neuropathies that progressively damage the optic nerve. In most cases, this damage occurs as a result of elevated intraocular pressure (IOP), although there is also normotensive glaucoma, in which the IOP remains within normal ranges yet the nerve continues to deteriorate.
The clinical outcome is always the same: loss of peripheral vision that progresses towards the centre if left untreated. By the time a patient notices this loss, it is usually years after the damage first began.
According to the World Health Organisation, glaucoma causes bilateral blindness in more than 7.7 million people worldwide and is the leading cause of irreversible blindness globally. In Spain, the prevalence stands at around 3% of the adult population, according to the Spanish Glaucoma Society, and approximately 50% of those affected are unaware of their diagnosis.
The risk factors most commonly observed in clinical practice are:
- Family history of glaucoma (the risk in first-degree relatives is ten times higher)
- High myopia, particularly above 6 dioptres
- Ocular hypertension without established nerve damage
- Diabetes mellitus and cardiovascular diseases
- Prolonged use of corticosteroids, whether in the form of eye drops, oral medication or inhalers
- Aged over 40 (prevalence increases with each decade)
- Previous eye injuries or surgery
Identifying these factors is the first step. The second is to check the condition of the optic nerve using a comprehensive diagnostic eye examination before any loss of vision occurs.
Glaucoma diagnosis at Dr Nowrouzi’s surgery
The diagnosis of glaucoma is not simply a matter of measuring eye pressure. An IOP of 22 mmHg may be normal in an eye with a thick cornea, or dangerous in another with a thin cornea. Dr Nowrouzi’s protocol assesses both the structure and function of the optic nerve from various perspectives.
OCT of the optic nerve and nerve fibre layer
The optical coherence tomography (OCT) It quantifies the thickness of the peripapillary nerve fibre layer and the macular ganglion cell layer with a resolution of micrometres. In clinical practice, this makes it possible to detect structural damage before it becomes apparent in the visual field, in some cases 5 to 8 years in advance. Longitudinal follow-up with OCT is the current standard for monitoring disease progression.
Computerised campimetry
The computerised campimetry assesses peripheral and central visual function. Modern equipment enables the detection of incipient scotomas, the classification of disease stage according to AGIS or Hodapp-Parrish-Anderson criteria, and the assessment of whether treatment is halting progression. In moderate or advanced glaucoma, perimetry guides therapeutic adjustments more than any other test.
Corneal pachymetry
The corneal pachymetry measures the central thickness of the cornea. A thin cornea underestimates the actual pressure: a patient with an apparent IOP of 18 mmHg may have a corrected IOP of 21 mmHg if their cornea measures 500 µm instead of the average of 545 µm. Without this information, the target pressure may be incorrectly set from the outset.
Gonioscopy
Gonioscopy visualises the iridocorneal angle and determines whether the glaucoma is open-angle or closed-angle. This classification is not merely a technicality: it completely determines the treatment. SLT is used in open-angle glaucoma. In narrow-angle glaucoma, a YAG laser iridotomy or lens extraction may be indicated.
Digital fundus photography
The digital retinography It documents the appearance of the optic nerve and allows for comparisons over time. The cup-to-disc ratio and analysis of the optic disc are classic signs of glaucomatous damage which, when assessed in a series of examinations, reveal whether structural progression is occurring.

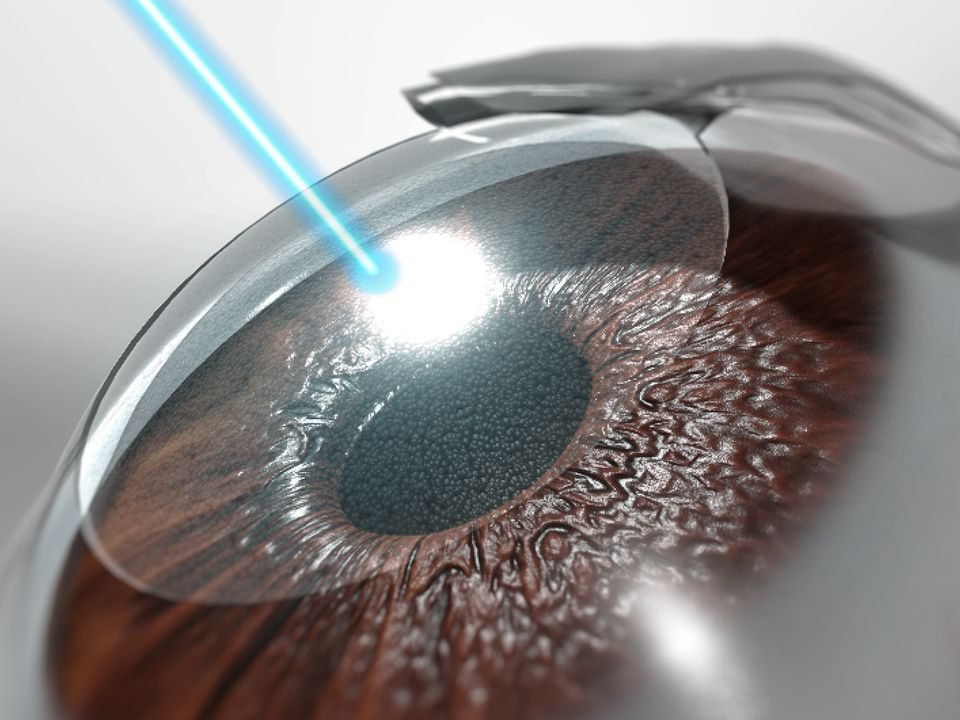
SLT laser treatment for open-angle glaucoma
Selective laser trabeculoplasty (SLT) is currently the first-line treatment for mild or moderate open-angle glaucoma recommended by the European Glaucoma Society. It does not require any incisions, does not cause scarring, and can be repeated if the response diminishes over time.
The mechanism is selective: the laser acts on the pigmented cells of the trabecular meshwork without damaging adjacent structures, thereby improving the natural drainage of aqueous humour and reducing IOP. Approved by the FDA in 2002, it has over twenty years of published clinical evidence.
One systematic review with meta-analysis published in PubMed It compared SLT with hypotensive eye drops as first-line treatment: the reduction in IOP was comparable between the groups, with a significantly lower rate of progression to surgery and a lower need for additional medication in the SLT group.
This clinical equivalence, coupled with a very favourable safety profile, explains why SLT has gained ground over long-term medical treatment in many patient groups.
The advantages over long-term medical treatment are clear:
- An outpatient procedure lasting 10–15 minutes, using anaesthetic eye drops
- No incisions, no general anaesthetic, no time off work
- Without the side effects associated with long-term use of eye drops: irritation, dryness, preservative toxicity
- May be repeated in cases where the initial response subsides
- Improves adherence to treatment: the patient does not have to rely on taking medication every day
Information on the Advanced glaucoma treatments without invasive surgery available at Dr Nowrouzi’s surgery. For patients who are intolerant to preservatives or who prefer to minimise their medication intake, the medical laser treatment It is an alternative with consistent clinical support.
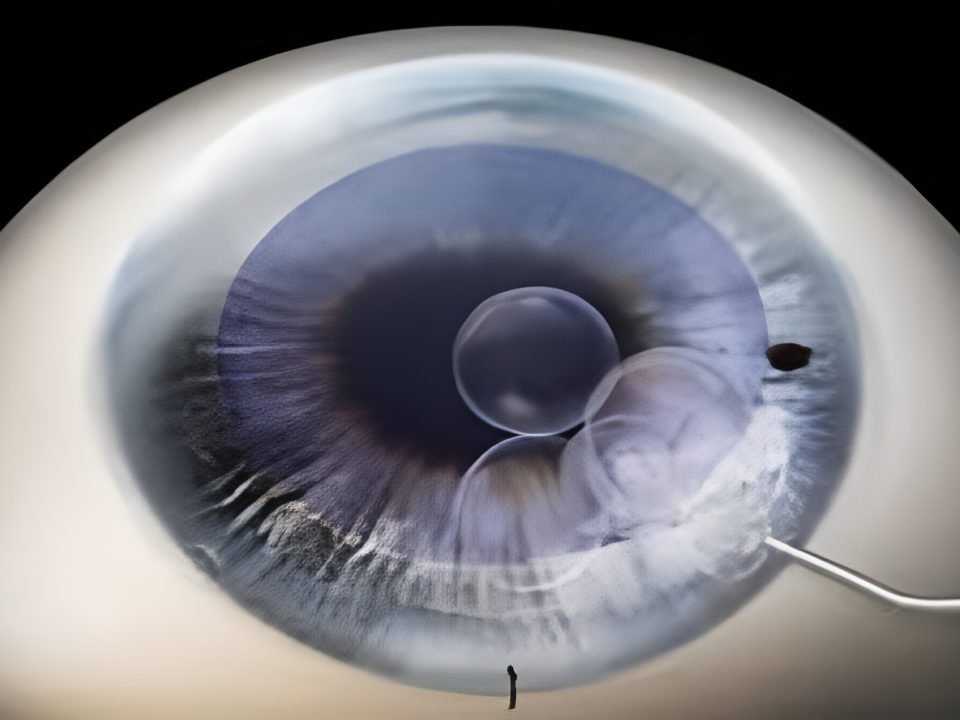
MIGS surgery: minimally invasive treatment for glaucoma
MIGS (Micro-Invasive Glaucoma Surgery) techniques have brought about a significant change in the surgical management of glaucoma over the last decade. The concept involves reducing intraocular pressure (IOP) via ab interno micro-incisions, without the risks of complications associated with trabeculectomy or conventional drainage valves.
According to a clinical review published in PMC, MIGS techniques using devices such as the iStent inject W or the Hydrus Microstent achieve reductions in IOP of 15% to 50%, alongside a reduction of between 0.4 and 1.8 antihypertensive drugs. When combined with cataract surgery, the results outperform cataract surgery alone in all pressure control parameters.
IOLs are particularly useful in mild or moderate glaucoma and are often combined with lens surgery when the patient has cataracts or a significant refractive error.
MIGS combined with cataract surgery in Marbella
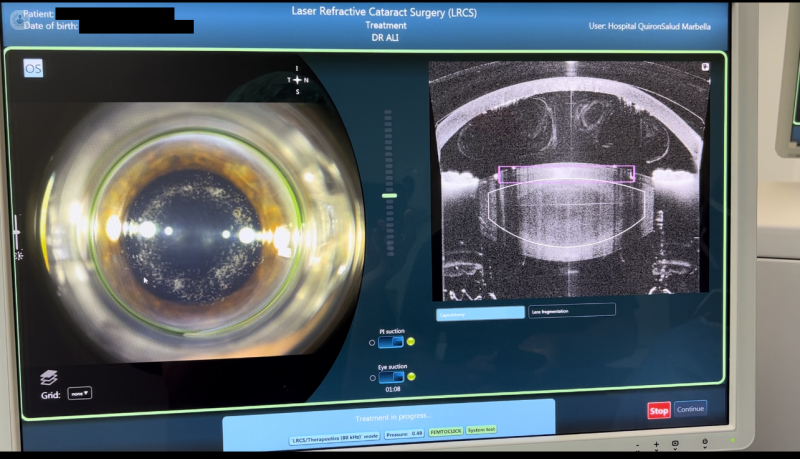
The femtosecond laser cataract surgery In a patient with glaucoma, this can be combined with the implantation of a MIGS microdevice during the same surgical procedure. The clinical rationale is straightforward: the incision required for phacoemulsification is utilised, the total operating time is reduced, and the patient recovers from both conditions at the same time.
Depending on the type of glaucoma, the target pressure and the condition of the iridocorneal angle, the choice of device varies between trabecular meshwork bypass (iStent inject), canaloplasty with Hydrus, ab interno goniotomy (GATT) or other options. Planning involves advanced ocular biometry, pre-operative gonioscopy and the setting of a target pressure based on the stage of optic nerve damage as assessed by OCT and perimetry.
Premium intraocular lenses in patients with glaucoma
Many patients with glaucoma also have cataracts or presbyopia requiring spectacles. Advances in biometrics and lens design have expanded the possibilities for visual correction for this patient group as well.
The Premium intraocular lenses (trifocal, EDOF, toric) simultaneously correct myopia, hyperopia, astigmatism and presbyopia. In cases of mild or moderate glaucoma with preserved functional visual fields and stable intraocular pressure (IOP), the implantation of a premium lens is a viable option that should be considered based on the condition of the optic nerve and the patient’s visual expectations.
In cases of more advanced visual field loss, lens selection generally favours monofocal or EDOF lenses, which are less contrast-dependent. Diffractive lenses may subjectively reduce visual quality when there is significant visual field loss.
The correction of presbyopia and eyestrain In the context of glaucoma, this is not always possible, but it does not automatically rule out the patient either. Eligibility is determined on a case-by-case basis, based on up-to-date OCT and perimetry data.

Dr Nowrouzi’s career and qualifications in eye surgery
Dr Ali Nowrouzi is Head of the Ophthalmology Department at Quirónsalud Palmones Hospital and sees patients at four centres on the Costa del Sol: Clínica Premium Marbella, Quirónsalud Marbella, Hospital Ochoa and Hospiten Estepona.
His FEBOS-CR certification (Fellow of the European Board of Ophthalmology, sub-specialising in refractive surgery) attests to the most rigorous European training in ocular microsurgery. A co-author of over 100 international scientific publications, he participates as a surgical demonstrator at conferences ESCRS and ASCRS, where the “Dynamic Pre-ocular Reconstructive Rejuvenation” technique has been demonstrated in live presentations.
The combination of advanced diagnostics, SLT, MIGS surgery and premium lenses within a single professional profile is precisely in line with Dr Nowrouzi’s training and surgical practice. Further information can be found at the Dr Ali Nowrouzi’s full career history in the About Us section.
Warning signs: when to seek a glaucoma assessment in Marbella
Some cases of glaucoma are detected during routine check-ups, with no prior symptoms. Others come to the clinic because of a specific symptom. It is advisable to seek a specialist assessment in either of these situations:
- Family history of glaucoma or blindness caused by an eye condition in first-degree relatives
- Previous diagnosis of ocular hypertension (IOP > 21 mmHg without established structural damage)
- High myopia of more than 5–6 dioptres
- Frequent use of corticosteroids, either as eye drops or systemically, for more than three months
- Aged over 50 and not having had an eye test in the last two years
- Blurred peripheral vision or a sensation of a foggy area at the sides of the field of vision, even if intermittent
- Halos or blurred vision around lights at night, particularly if it is monocular
Detection before functional damage occurs makes all the difference between controlling the disease and managing a loss that is already irreversible. You can also find information on diseases of retina and optic nerve available at the surgery.
Frequently asked questions about glaucoma in Marbella
Is there a cure for glaucoma? Not in the sense of reversing damage that has already occurred: the optic nerve does not regenerate. However, glaucoma can be managed. With appropriate treatment, most patients retain their functional vision for decades. The aim of treatment is to halt the progression of the disease, not to reverse existing damage.
Does SLT cause pain or require recovery? No. It is carried out in the surgery using anaesthetic eye drops and takes between 10 and 15 minutes. Some patients report mild discomfort for a few hours after the procedure. It does not require time off work or any special restrictions on activity.
When is MIGS combined with cataract surgery? When a patient has mild or moderate glaucoma and cataracts that are affecting their vision, combined surgery is an effective option: the lens and IOP are treated during the same surgical procedure. The indication depends on the type and stage of the glaucoma, the condition of the iridocorneal angle and the target pressure set.
Can I have surgery for cataracts or presbyopia if I have glaucoma? It depends on the stage of the disease and how well the glaucoma is controlled. Stable optic neuropathy, with controlled IOP and preserved functional visual field, is not an absolute contraindication for lens surgery. Pre-operative assessment includes a recent OCT scan, perimetry and an individual risk assessment.
What is the difference between open-angle and closed-angle glaucoma? Open-angle glaucoma, the most common form, is characterised by elevated IOP due to resistance to drainage in the trabecular meshwork. Closed-angle glaucoma occurs when the iris physically blocks the angle and can lead to acute attacks with severe pain and sudden loss of vision. The therapeutic approach differs in each case.
What tests are carried out during the initial assessment for glaucoma? The initial consultation includes tonometry, examination of the optic nerve with pachymetry, and assessment of the angle. Depending on the suspected diagnosis, OCT of the optic nerve and perimetry are also carried out. In the diagnostic tests page You can view full details of the available scans.
Which health insurance schemes does Dr Nowrouzi’s practice accept? The practice works with the main private health insurers. To confirm specific cover for glaucoma tests or available treatments, we recommend that you contact the practice directly before your appointment.
Book your glaucoma screening in Marbella
If you have risk factors for glaucoma or have not had a comprehensive eye examination in the last two years, you should take action before symptoms appear. Dr Ali Nowrouzi carries out comprehensive examinations of the optic nerve using OCT, perimetry and pachymetry at his centres in Marbella, Quirónsalud and Hospiten Estepona.