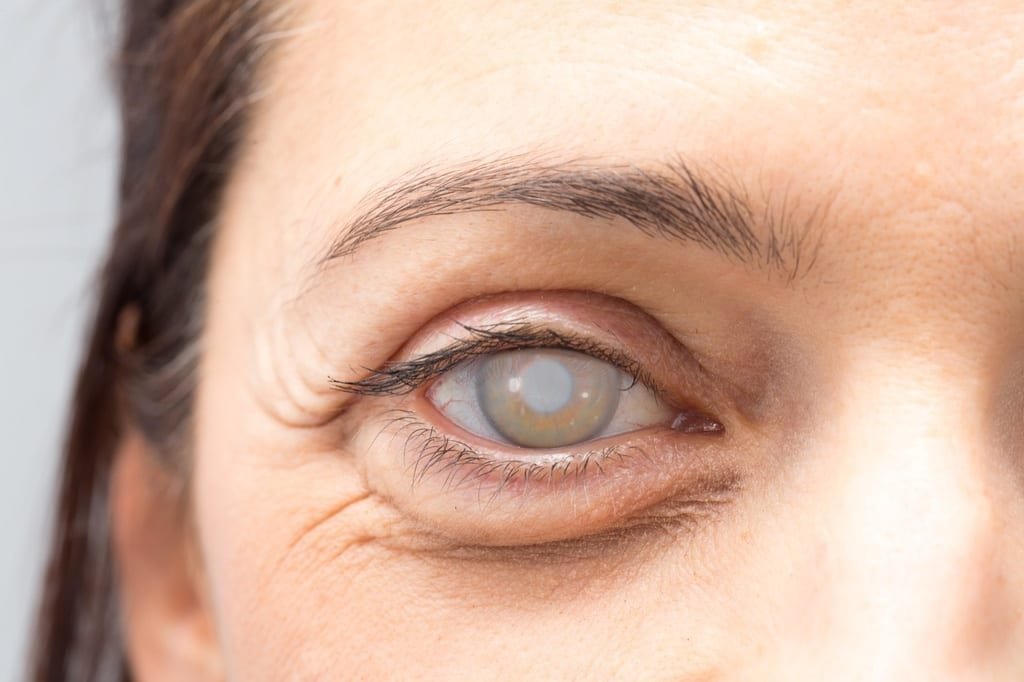
The waterfall does not give any urgent warning. It comes on slowly: first the colours appear washed out, then car headlights at night become unbearable, then you can no longer read with the light that used to suffice. Many patients endure months - or years - without knowing whether it is time for surgery, or whether they can still wait.
The short answer: you don't have to wait until you can't see at all. The recommendation to wait until the cataract is “mature” has become obsolete. Today it is advisable to intervene before reaching that point, because the more advanced the cataract is, the harder the lens becomes and the more complex the surgery becomes.
The long answer - when exactly, what signs to look for, what happens if you have diabetes or glaucoma, and what surgery looks like when it's done at the right time - is what this article explains.
Checklist: is it your time to operate?
Before going into medical criteria, answer these questions. If you tick three or more, it is worth asking for an assessment:
- Do you have difficulty reading even if you have recently changed your glasses?
- Do car headlights at night dazzle you and create halos?
- Do you see the colours dull or with a yellowish tinge?
- Do you find it difficult to recognise faces at a distance?
- Have you stopped driving at night because of visual insecurity?
- Has your visual acuity changed several times in the last year even though you have updated your prescription?
- Does reading or screen work make you more tired than usual?
It's not a diagnosis, it's a sign that the cataract may be affecting your daily life more than you think.
What determines when to operate: quality of life, not figures
The decision to operate is not based solely on the degree of lens opacity, but on how the cataract affects the patient's day-to-day life. Two people with the same density of cataract may have very different surgical indications: a professional driver needs vision that a sedentary pensioner may still have.
The important thing is not to operate before anyone else, but to operate when vision already interferes with quality of life or safety when driving or working. This is the golden rule that specialists use, and it is more useful than any visual acuity figure in an optometric test.
Why functional criteria matter more than degree of opacity
A patient with a moderate cataract who drives 300 km per week has a clear surgical indication. A patient with a more advanced cataract who lives a visually undemanding life may be under observation for a longer period of time. The best time to operate is when the patient begins to notice that his or her daily life is limited. The earlier the operation is performed, the better the adaptation and the better the final result.
Signs that it is no longer worth waiting
There are specific situations in which prolonging the wait is no longer reasonable.
Risk of falls and accidents
Blurred vision in older people increases the risk of trips and falls. If the cataract already affects depth perception or twilight vision, the indication for surgery becomes a priority - not for aesthetics, but for safety.
The lens hardens over time
Over the years, the lens loses elasticity and hardens. This makes its removal at the time of surgery technically more complex and requires more energy inside the eye, with the internal structures becoming more fragile. A dense cataract marginally increases surgical risks and lengthens recovery.
Increased intraocular pressure
Waiting too long can lead to other eye problems, such as increased intraocular pressure or inflammation. In patients predisposed to glaucoma, this adds another reason not to delay the procedure once it has been recommended by the specialist.
Cataract blocks tracking of other diseases
Sometimes it is necessary to remove the cataract so that the specialist can see the back of the eye clearly. This may be essential to treat other problems such as diabetic retinopathy or macular degeneration. In these cases, surgery is not only to improve direct vision, but also to treat the underlying retinal pathology.
Special cases: when to operate if you have another eye disease
This is the block that patients are most concerned about and that the usual articles deal with in a superficial way.
Cataracts with diabetes
Diabetic patients develop cataracts more frequently and at an earlier age. High blood glucose levels can cause structural changes in the lens over time that accelerate its opacification. The good news: most can be operated on with a good prognosis.
A diabetic patient is usually a good candidate for surgery when the cataract significantly limits vision, when the eye has no retinal disease that contraindicates the procedure, and when the general metabolic status allows safe progress. What is essential is that the specialist differentiates how much visual loss comes from the cataract and how much comes from retinopathy or macular oedema - because surgery resolves the former, but not the latter.
Cataracts with glaucoma
In patients with glaucoma, combined surgery for both pathologies can be performed. In these cases, a monofocal or EDOF lens is usually recommended, and in some specialised centres it is performed with specific techniques that address both conditions in the same session. The indication depends on the degree of optic nerve involvement and whether the glaucoma is well controlled.
Cataracts with macular degeneration
Cataract surgery does not restore vision lost due to macular degeneration or diabetic retinopathy. This is important to understand before the operation: the cataract resolves, but if there is macular damage in the background, the vision recovered will depend on the state of the retina. With advanced macular degeneration, multifocal lenses are contraindicated and it is recommended to opt for monofocal or EDOF lenses.
Cataracts in young people: causes and different criteria
Not all cataracts are senile. Trauma to the eye, even mild, can alter the structure of the lens and cause progressive opacification. Prolonged use of corticosteroids - whether in tablets, inhalers or eye drops - is another common cause. Metabolic diseases such as diabetes, which alters the internal composition of the lens, also play a role.
In these cases the functional criterion is applied in the same way, but with nuances: the young patient has more years of visual life ahead of him/her, which makes the choice of intraocular lens more relevant and the preoperative period more critical.
Posterior subcapsular cataracts, often caused by prolonged use of oral corticosteroids, can cause a marked drop in vision and progress rapidly in a few months - so these patients need to be monitored more closely than a slowly progressing senile cataract.
What is no longer valid: the myth of the “mature waterfall”.”
For decades it was repeated that you had to wait until the cataract was very advanced before intervening. Ideally, the intervention should be carried out when the person's vision starts to become limited and affects their lifestyle - not when they can hardly see at all.
To benefit from the most modern techniques, it is not necessary to lose vision completely: it is more beneficial to operate when the cataract is not very advanced, which allows it to be removed with greater precision and less risk. Current phacoemulsification and femtosecond laser techniques make it possible to operate at any stage.
When to advance surgery even if vision is acceptable
There are situations where it makes sense to operate before vision is clearly poor.
There are patients in whom the cataract is not the main cause of the visual limitation, but rather the prescription they can no longer tolerate comfortably - high hyperopia, myopia or advanced presbyopia. In these cases, even if the lens opacity is mild, surgery may be considered to improve overall visual quality and reduce dependence on glasses.
The indication is also brought forward when:
- The profession requires high visual precision (driver, pilot, surgeon, artist).
- There is a retinal pathology that requires a clean fundus examination.
- Patient has glaucoma and combined surgery improves intraocular pressure control.
What surgery looks like when it's done at the right time
Cataract surgery is an outpatient procedure that does not require hospitalisation. It lasts between 15 and 30 minutes per eye and is performed with local anaesthesia in drops, without injections or hospitalisation.
The usual rule is to operate on the eyes separately with an interval of 10 to 15 days: one eye is operated on, the result is assured, and then the other is operated on.
Types of intraocular lenses: the decision that has the biggest impact on outcome
The choice of lens is as important as the time of operation. There are four main families:
Monofocal - Correct distance vision. They usually require glasses for near vision. They are covered by Social Security. The price in a private clinic is around €1,800 per eye.
Multifocal and trifocal - They allow you to see at various distances without glasses. They are the most demanded by patients with an active life. They are contraindicated if there is macular degeneration or advanced retinopathy.
EDOF (extended range) - A middle ground between monofocal and multifocal. They offer good distance and intermediate vision with fewer night halos. Indicated for patients with associated mild ocular pathology.
O-rings - They correct astigmatism simultaneously. They are combined with any of the previous types.
The total price range in Spain, depending on the lens and centre, ranges from €1,200 to €3,500 per eye. Social Security covers monofocal lens surgery, but there is a waiting list.
Recovery: faster than people expected
After 72 hours, most patients are able to drive, work in an office and lead a normal life without any sudden efforts. Vision stabilises definitively after about a month, when the final prescription is prescribed - in many cases with premium lenses, without the need for glasses.
Femtosecond laser cataract surgery: state-of-the-art precision
In the most advanced centres, cataract surgery can be performed with femtosecond laser technology, a significant evolution over the conventional technique. This system automates key steps of the surgery - such as corneal incisions, lens opening and cataract fragmentation - with millimetre-accurate and highly reproducible precision, reducing the energy required inside the eye and optimising the safety of the procedure.
Dr. Ali Nowrouzi is one of the pioneers in Marbella in the use of this technology, being a specialist in laser surgery and offering his patients treatments with state-of-the-art equipment combined with premium intraocular lenses.
This not only eliminates cataract, but also improves overall visual quality, correcting refractive errors and reducing dependence on glasses with a highly personalised approach.
There is no maximum age for cataract surgery
There is no maximum age for cataract surgery. People aged 85, 90 or even older can be operated on as long as they are in good general health, do not present serious medical risks and are able to cooperate with basic instructions during the operation. The surgery takes less than 30 minutes, with topical anaesthesia and without hospitalisation.
What assessment you need before deciding
Before operating, a well-done preoperative procedure makes the difference between an excellent and a mediocre result. The specialist must perform:
- Ocular biometryto calculate the exact power of the intraocular lens
- Corneal topographyto detect astigmatism or lens-conditioning irregularities
- Macular OCTto rule out retinal pathology limiting the visual outcome
- Visual simulationto allow the patient to see the expected result before deciding
- Optic nerve assessmentif there is suspicion of associated glaucoma
Dr. Ali Nowrouzi operates in Marbella (Quirónsalud, Hospital Ochoa and Hospiten Estepona) and performs all assessments and surgeries personally. With more than 4,000 operations and top international certifications - FEBOS-CR by the European Board of Ophthalmology and recognition among the 100 best refractive surgeons in the world by the WCRS - he is one of the most experienced cataract specialists on the Costa del Sol.
One patient summed it up well in his Google review: “After years with virtually no vision, I decided to trust Dr. Nowrouzi to perform the trifocal intraocular lens procedure, and I couldn't be more grateful. From the first consultation, he explained everything to me clearly, conveying confidence and professionalism. The surgery was quick, painless and with a surprisingly easy recovery..” The first assessment is free, in Spanish and English, and there is no waiting list.
FAQs - Frequently Asked Questions
When is the right time to operate on cataracts?
When the cataract limits everyday activities such as reading, driving or seeing clearly in normal light conditions. There is no universal visual acuity figure: the criterion is functional, not just clinical. If you tick three or more items on the checklist in this article, ask for an assessment.
Is it dangerous to wait for cataract surgery?
Cataracts continue to develop progressively. Excessive delay, once surgery is recommended, can result in complications and increase the surgical risk. The lens hardens over time and the procedure becomes more technically demanding.
Do I have to wait until the cataract is very advanced?
No. This recommendation has been discarded for years. Current techniques allow cataract surgery at any stage, and the results are better when the lens is not yet very dense.
At what age is cataract surgery usually performed?
From the age of 50-55 it is not uncommon to detect a certain degree of cataract, although it is from the age of 65 onwards that they are present in more than 50% of people. In patients with diabetes, eye trauma or prolonged treatment with corticosteroids, they may appear much earlier.
Can both eyes be operated on at the same time?
It is not recommended. The usual practice is to operate on one eye and, after 10 to 15 days, to operate on the second eye. This reduces the risk of bilateral infection and allows the lens of the second eye to be adjusted according to the result of the first eye.
Can I take advantage of cataract surgery to remove my glasses?
Yes, using multifocal or trifocal lenses implanted during the same surgery, it is possible to correct tired eyesight, myopia or astigmatism and achieve independence from glasses. The specialist will assess whether you are a candidate according to the state of your retina and your visual needs.
Can I have cataract surgery if I have glaucoma or diabetes?
In most cases, yes. Patients with glaucoma, diabetes or macular degeneration can be operated on, although the visual result depends on the underlying pathology and the type of lens recommended will be different. A complete preoperative study that evaluates both conditions is essential.
How long is the recovery time after cataract surgery?
After 3 days most patients are able to drive and resume office activities. Vision stabilises definitively after about a month, when the final prescription is prescribed.
Do cataracts come back after surgery?
No. The cataract is physically removed and does not recur. Between 10 and 15% of patients may develop an opacity in the posterior capsule of the lens over the next two years, which resolves on an outpatient basis with YAG laser in a few minutes.
If you have diagnosed cataracts and you don't know if it's your time, or you have been putting off the decision for some time, the most useful thing is not to read on - it's a personalised assessment with a specialist who will tell you exactly how your cataract is, if you have any associated pathology that conditions the indication, and which lens is best for you.
Dr. Ali Nowrouzi performs the first consultation free of charge in Marbella. No waiting list. Attention in Spanish and English. Complete diagnosis with biometric study, topography and visual simulation included.
To assess the appropriate timing of the intervention, we conducted a ocular biometry for the calculation of the lens and a Pre-operative OCT to assess the condition of the retina before surgery.